VALVE PROSTHESIS
MECHANICAL PROSTHESIS
- In use since 1960s
- Divided into caged-ball, disc (monodisc) and bileaflet valves
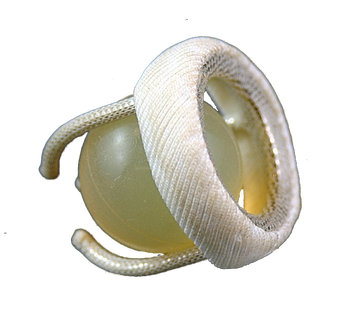
Caged-Ball Valves

Caged-ball valve Starr–Edwards (aortic model 1260)
|
Caged-Ball Valves Starr-Edwards valve
|

Caged-ball valve Smelo–Cutter
|
Caged-Ball Valves Smeloff–Cutter valve
|
Disadvantage:
- Frequent thromboembolic complications
- Efforts to reduce this has led to development of the cloth-covered caged-ball valves
- Best valves were the Braunwald–Cutter valve and Cloth-covered Starr–Edwards valve
- Struts and the ring were covered with polypropylene into which endothelium grew within several weeks or months after implantation
- Thereby, except for the ball, blood did not contact a foreign surface
- Limited reduction in the incidence of thromboembolic events and haemolysis was achieved but remained limited to the first months or few years after implantation.
- Tearing of the cloth covering occurred as a result of hardness and disparity between the ball and the endothelialized covering
- This initiated thrombus formation with subsequent thromboembolic events
- Also caused clinically significant haemolysis
- All prompted reoperation and valve reimplantation

Cloth-covered Starr–Edwards valve
Braunwald–Cutter valve
|
Caged-Ball Valves Cloth-covered Starr–Edwards valve
Caged-Ball Valves
Cloth-covered Braunwald–Cutter valve
|
Disc Valves
Can be divided into Non-tilting and Tilting Disc valves
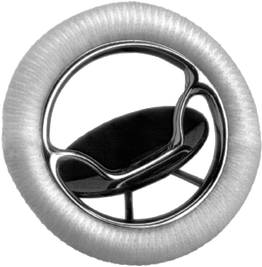
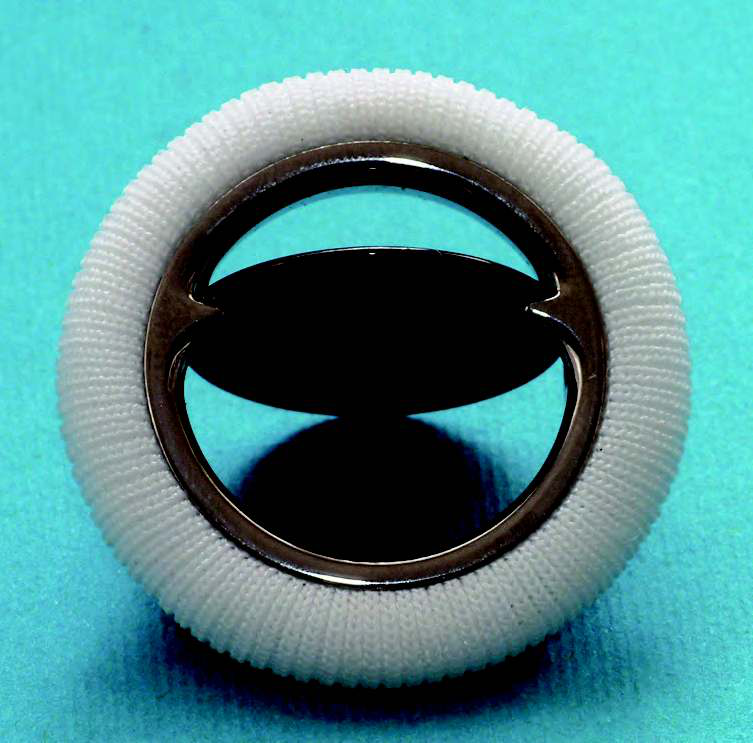
Non-Tilting Disc Valves
Can be divided into Non-tilting and Tilting Disc valves
Non-Tilting Disc Valves
- Non-tilting disc valves were introduced into clinical practice in the late 1960s into clinical practice.
- The closing component was a poppet that was held in a cage (open position) or obturated the ring (closed position)
- Best known valves:

Non-tilting disc valves
|
Non-tilting disc valves a) Beall b) Starr–Edwards |
Advantage:
Disadvantage:
- Low profile design
- Easier implantation
- Very little opening resistance
- Very short closure delay (hence very little regurgitation)
Disadvantage:
- Higher flow resistance
- Significant turbulence
- Frequent thromboembolic complications
- Higher haemolysis rate
Tilting Disc Valves
- Were the most-often implanted valves in the 1970s and 1980s.
- Precise knowledge of the tilting angle in monodisc and bileaflet valves is important for eventual diagnostics of the valve failure.
- Discs are radio-opaque and therefore fluoroscopy imaging can confirm their normal mobility or diagnose restricted range of motion, or even complete occluder blockade.
Disc valve Björk–Shiley
Disc valve Björk–Shiley
Standard type with at disc:
Standard type with at disc:
- The most commonly used valves In Europe .
- The First Model had a delrin disc, tilted up to 60°.
- Soon replaced by a the standard type with pyrolytic carbon at disc tilting up to 60°.
- Introduced in 1976.
- Has a significantly improved haemodynamics.
- Discontinued in the late 1980s because the inflow bar broke in some after 2–3 years of perfect performance, causing escape of the disc and acute valve regurgitation (can be lethal).
- Since then, the struts in all heart valves are not welded but manufactured from a single block of metal or alloy or from pyrolytic carbon.
- The latest Model.
- Introduced into clinical practice in 1982.
- The disc-housing system was changed and the angle of tilting was increased to 70°.
Disc valve Omniscience
|
Disc valve Omniscience
|

Disc valve Allcarbon–Sorin
|
Disc valve Allcarbon–Sorin
|

Disc valve Medtronic–Hall
|
Medtronic–Hall (originally Hall–Kaster)
|
The Ultracor–Aortech valves (developed in 1985), the tilting angle of which is 73° in the aortic model and 68° in the mitral model, have also been implanted.
Bileaflet Valves
Gained popularity since the mid-1980s
Currently are the most frequently implanted valves in the world
Different types but all based on the same or similar principle but differ in:
Gained popularity since the mid-1980s
Currently are the most frequently implanted valves in the world
Different types but all based on the same or similar principle but differ in:
- Angle of tilting.
- Design of the pivots.
- Material and shape of the sewing ring.
- Depth of the leaflets in their open position.
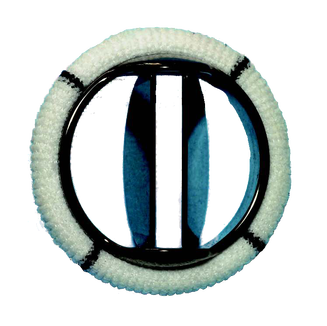
Bileaflet valve St. Jude Medical
St Jude Medical (SJM) valve:
SJM HP EOA = 2.03cm2
SJM Regent EOA = , 2.47cm2
- Best-known and most implanted mechanical bileaflet valve.
- In clinical practice in 1977 (SJM Standard).
- Semilunar leaflets open up to 85° and close at 30°, yielding a tilting range of 55°.
- SJM HP (hemodynamic plus, since 1992) and SJM Regent (since 1998) with a reduced sewing ring, which results in significant enlargement of the effective orifice area (EOA) (avoiding patient-prosthesis mismatch - PPM)
- EOA for Size 21-mm SJM is:
SJM HP EOA = 2.03cm2
SJM Regent EOA = , 2.47cm2
- SJM Regent 19-mm valve has an EOA of 1.84cm2 which is sufficient to prevent PPM in a patient with a body-surface area of 2cm2.

Bileaflet valve Sorin–Bicarbon Slimline
Bileaflet Bicarbon–Sorin
- Second most commonly implanted bileaflet valve.
- Manufactured since 1990.
- Semilunar leaflets are convex–concave shaped and tilt up to 80° and close at 20° .
- Sewing rings Fitline or Slimline (suitable for small annuli).
- Overline (intended solely for supra-annular implantation).
- The same mechanism, but a different sewing cuff material, is typical for the Edwards MIRA valve (since 1997).
CarboMedics Valves
- In clinical use since 1986.
- Semilunar leaflets tilt up to 78° and close at 25°, which gives a tilting range of 53°.
Carbomedics Standard Mitral Valve


|
CARBOMEDICS OPTIFORM: Adaptable for:
CARBOMEDICS R (Reduced)
|

|
Carbomedics Top Hat
|

|
CarboMedics Orbis:
|

|
ATS Medical:
|
- Medtronic Advantage has, since 2003, A modification for supra-annular implantation named Medtronic Advantage Supra.
- The most recent bileaflet valve introduced into clinical practice is the valve CardiaMed.
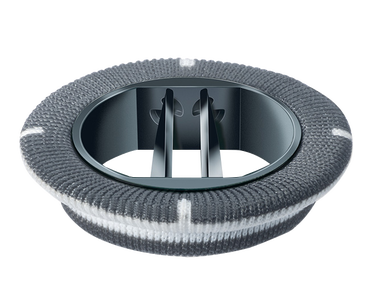
oN X VALVE
On-X Life Technologies, Austin, TX
- Bileaflet valve
- Constructed completely from pyrolytic carbon.
- Lack of silicon doping in the carbon construction potentially decreases its thrombogenicity.
- Has a tall flared inlet that increases the orifice area and decreases the ability of retained valve tissue to interfere with the opening and closing mechanisms.
- Has a stasis free pivot that allow the valve to wash out itself.
- Has a 90-degree leaflet opening which provides improved laminar flow and reduce turbulence.
- Available is three different sewing rings:
- Standard:
- Aortic: sizes from 19 to 27/29 mm
- Mitral: sizes from 23 to 31/33 mm.
- Conform X: has a more flexible sewing ring.
- Aortic: sizes from 19 to 27/29 mm.
- Mitral: only one size that fits an annular size ranging from 25 to 33 mm.
- Anatomic:
- Designed to for the contours of the aortic valve annulus.
- Sizes from 19 to 27/29 mm.
- Standard:
- PROACT Trial ( Prospective Randomised On-X Anticoagulation Clinical Trial)
- Compared low dose Warfarin plus low dose aspirin (81mg) to standard warfarin.
- The first showed a significantly lower major and minor bleeding rates.
- The incidence of stroke, TIA, total neurologic events and all cause mortality were similar

ON X Standard Mitral

Ascending Aortic Prosthesis - CryoLife, Inc.