surgical EXPOSURE
Median sternotomy
- Exposes the anterior layer of the mediastinum and pericardium.
- Must be performed strictly in the mid-line.
- Para-median incision is a significant risk for sternal instability.
- A linear incision is made between two landmarks, the supra-sternal notch and the xiphoid process.
- For better cosmetics, the incision is started just above the sternal angle.
- Subcutaneous fat and pre-sternal fascia are divided using electrocautery.
- The linea alba us divided inferiorly for 1-2 cm.
- The mid-line is verified by examining the width of the sternum using two fingers at the 3rd or 4th intercostal space with attention to the insertion of the pectorals major muscles.
- The mid-line is marked by electrocautery.
- Blunt dissection behind the xiphoid process to free the pericardial and pleural attachment to the sternum. This must be avoided in redo sternotomy as there is a risk of cardiac injury due to post operative adhesions.
- The Sternum is divided in a cranio-caudal or caudo-cranial direction by a reciprocating saw along the marked mid-line exerting a gentle lift to avoid catching substernal structures with the saw blade.
- Haemostasis is achieved by cauterizing the periosteal surfaces of the sterum and slective application of bone wax
|
Vancomycin Paste:
|

|

|

|
Cardiac Exposure
or due to extensive adhesions to the pericardium
- Right auricle: in some cases, the aurile reaches over the sternocostal surface and may even
cover the pulmonary root, especially true in the presence of tricuspid insufficiency with
extensive dilatation of the right atrium may be present
- First, the epericardial fat tissue; an embryological remnant of the thymus, must be dissected down to the fibrous layer of the pericardium.
- The thymus vein, which is almost always found and drains into the left brachiocephalic vein is a good indicator of the border between the left and right thymus lobes, identified and ligated
- The pericardium is exposed up from the brachiocephalic vein down to the diaphragm.
- The pericardial incision should be initiated at the inferior part of the pericardium, approximately two finger-breadths over the diaphragm.
- Using electrocauterization, the incision is extended cranially toward the left brachiocephalic vein.
- Reaching the base of the heart, the incision must continue over the groove positioned between the aorta and the pulmonary root.
- At this stage, two very important structures of the heart are vulnerable to damage:
or due to extensive adhesions to the pericardium
- Right auricle: in some cases, the aurile reaches over the sternocostal surface and may even
cover the pulmonary root, especially true in the presence of tricuspid insufficiency with
extensive dilatation of the right atrium may be present
- The pericardial incision terminates at the level of the aortic arch, just inferior to the origin of the brachiocephalic artery
- Two horizontal extensions at the inferior end of the vertical incision just over the diaphragm must be performed (leaving a narrow rim of pericardial tissue may be beneficial in redo surgery to facilitate identification during adhesiolysis).
- The right-side incision is extended in a diagonal manner to the right, toward the inferior vena cava, and the left-side incision is extended left toward the apex of the heart

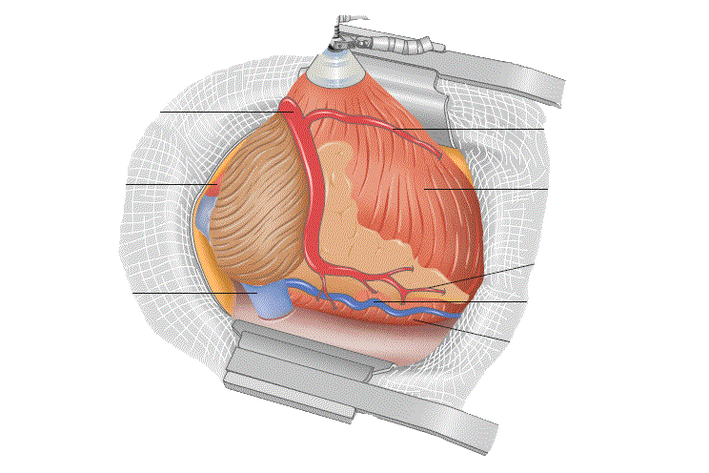
Exposure of the pericardium (solid line indicates the pericardial incision)
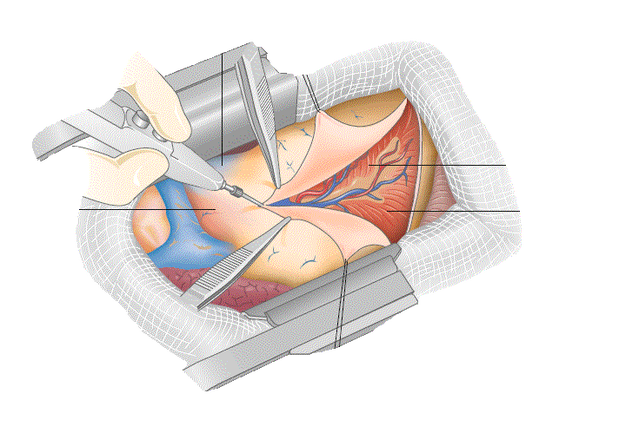
Pericardial incision
- Pericardium edges are fastened to the spreader, exposing the sternocostal surface of the heart.
- The pericardial cavity should then be inspected for fibrous strings, potential adhesions, or extensive fluid accumulation, which may elicit a different pathological processes in the pericardial cavity.
- Normally, about 15 ml of serous pericardial fluid may be found at the apex.

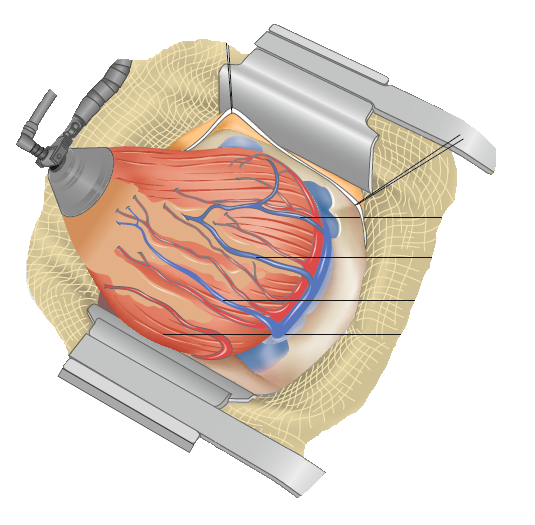
Sternocostal surface of the heart
The Vagus and Phrenic Nerves:
- The vagus and phrenic nerves traverse the length of the pericardium.
- They are well lateral mediastinal structures.
- The phrenic nerve on each side passes anteriorly to the lung hilum.
- The vagus nerve courses posteriorly to the hilum of the lung .
The Phrenic Nerve:
- It passes close to the IMA near the thoracic inlet exposing it to injury by:
- direct injury during IMA harvest.
- by avulsion of the pericardiophrenic artery with excessive traction on the chest wall.
- Dissecting part of the pericardium to be used as a patch.
- During pericardiectomy.
- The use of topical cooling within the pericardial cavity may induce cold injury to the nerve.
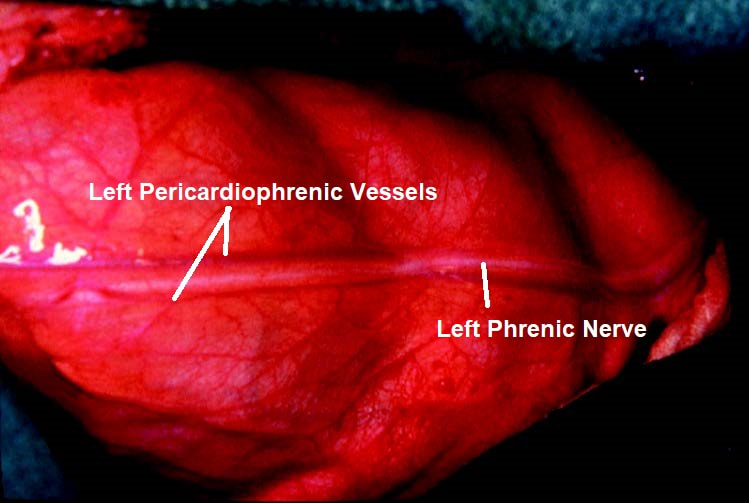
The course of the left phrenic nerve over the pericardium.
(View from Let Lateral Thoracotomy) 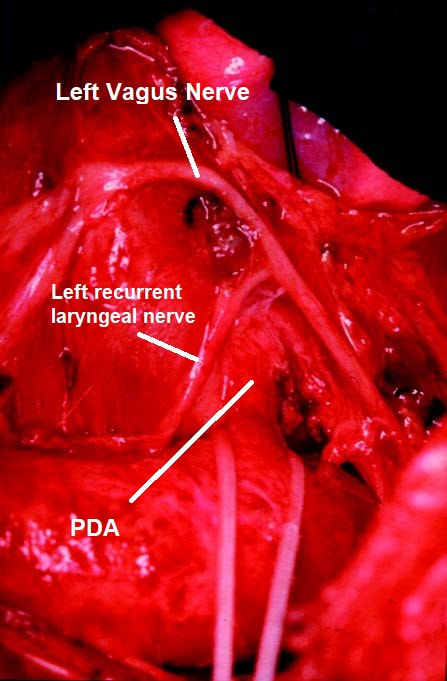
The left recurrent laryngeal nerve passing around a PDA.
|
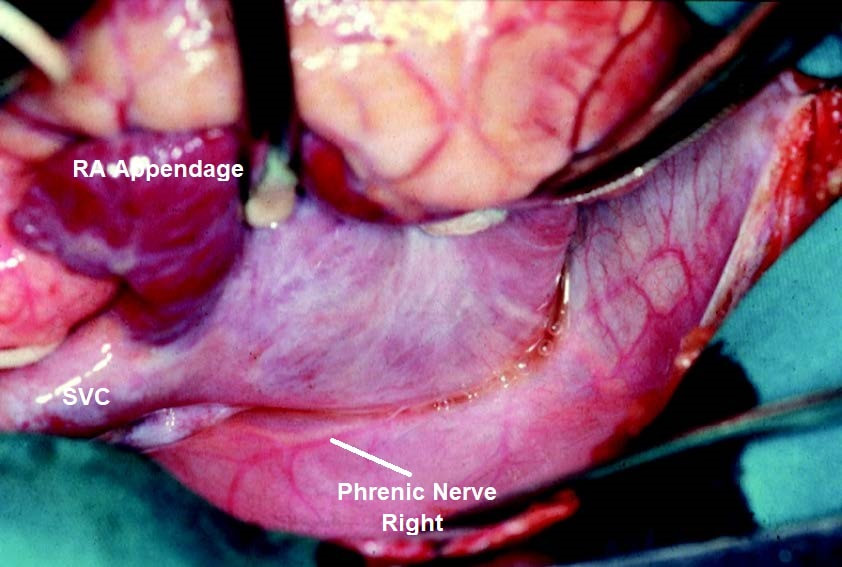
The right phrenic nerve seen through the pericardial reflection.
(View from Median Sternotomy) 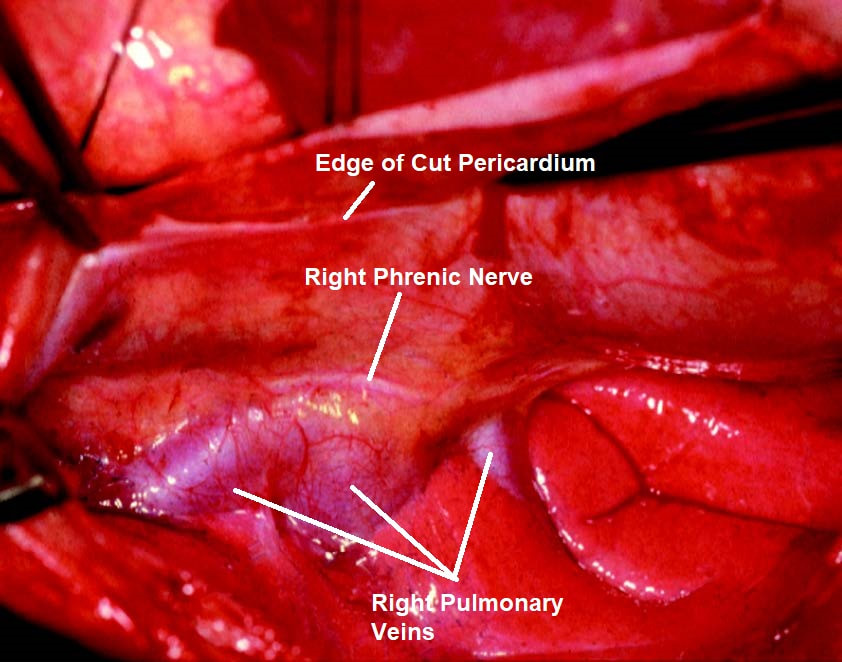
The right phrenic nerve in relation to the right
pulmonary veins. (View from Median Sternotomy) |
The Sternocostal Surface:
- The sternocostal surface of the heart comes into view in this exposure
- At the base, the heart from the right the right auricle covers the right aspect of the aortic root.
- To the left and superior of the ascending aorta, the pulmonary root may be found.
- The superior vena cava is just behind and lateral to the ascending aorta.
- The majority of the aortic root is just behind the posterior wall of the infundibulum.
- At the ventricular part of the heart, almost the whole sternocostal aspect is represented by the right ventricle; the left ventricle is seen only in the area near to the apex
- Because of the physiological left rotation of the whole heart in this aspect, only the middle and distal segments of the LAD can be seen
- Lifting the left heart by placing a coiled operating cloth into the left pericardial hemicavity, half of the entire course of the LAD and the proximal part of the Cx may be seen.
- The LAD runs over the anterior interventricular groove on the left side of the anterior cardiac vein.
- With extensive epicardial fat collection, the position of the artery may be difficult to identify.
- A smooth groove in the fat tissue just over the artery may indicate its position (not an absolute land-mark)
- Finding the artery may be particularly difficult when it is in the intramural position.
- Concomitant vein in some cases runs just over the artery, mimicking the course of the LAD; the anterior cardiac vein may be bypassed as a target artery
RCA AND RIGHT LATERAL VIEW
Exposure of right coronary artery and crux cordis
- The heart is then rotated to the left side, exposing the posterior part of the RCA (including the PDA)
- This is achieved by placing pure string sutures or with the aid of special suction devices
- The diaphragmal surface of the RV,the posterior interventricular sulcus and the nearby part of the left ventricle just near are thus explored.
- This exposition is appropriate for revascularization of the proximal RCA, the right marginal artery, and the PDA.
- The right marginal branch runs along the acute margin of the RV, toward the apex of the LV. It usually runs alone and without the concomitant vein and is easy to verify.
- The part of the RCA positioned in the diaphragmal part of the coronary sinus, is identified by searching the border between the epicardial fat tissue and the inferior border of the right atrium.
- The RCA is identified as an artery with a large diameter that runs in the epicardial fat tissue underneath the edge of the right atrium. It can be traced down to the crux, where it turns into the posterior descending sulcus
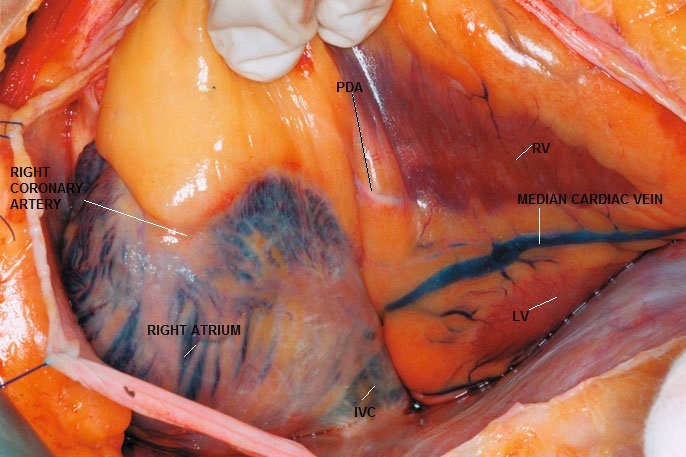
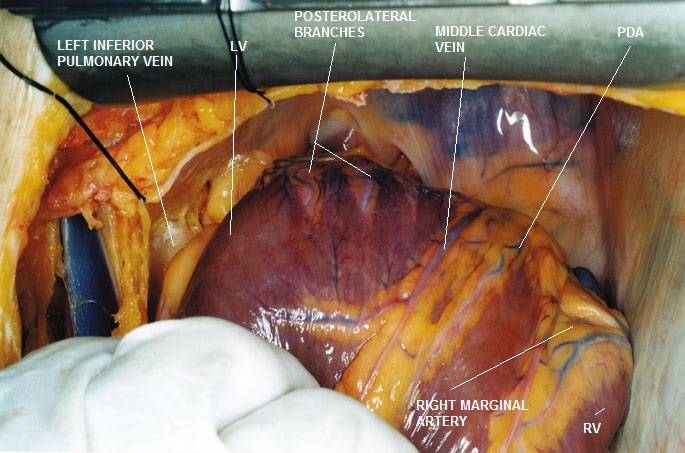
Exposure of the RCA and the posterolateral descending artery, right lateral view
- The ostium and proximal RCA may be found by lifting up the right auricle and retracting the infundibulum.
- The anterior part of the RCA appears in the right part of the coronary sulcus just inferior to the right atrium.
- The direction of the RCA identified in the initial part of the coronary sulcus also indicates the course of the RCA in the right coronary fossa. (Not always very easy to identify the artery due to extensive epicardial fat collection in the coronary sulcus)
- When the PDA branches off proximal to the crux, the artery is not always to be found in the posterior descending sulcus. It can run to the left or to the right of the posterior sulcus.
- The middle cardiac vein is found just lateral to the PDA (usually on the left side and superficial to it)
- Note: IVC enters RA just anterior and inferior to the diaphragmal surface of the heart
DIAPHRAGMATIC SURFACE
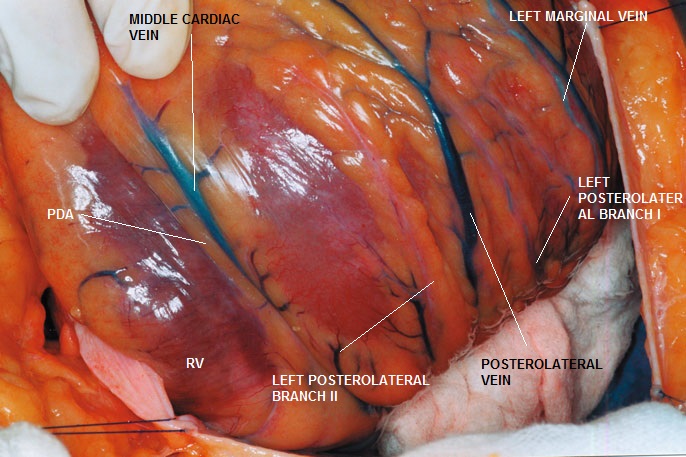
Diaphragmal surface of the heart, right lateral view
- In order to expose completely all vessels on the diaphragmal surface of the left and right ventricles, the apex must be lifted from the pericardium caudally and to the right. This maneuver may be completed without problem by using an apical suction device.
Diaphragmal surface of the heart, right superior view
- This exposure is superior for dissection and for bypassing of the left OM.
- This artery may be mistaken for the marginal branch of the RCA
- A very important landmark in this instance is the presence of the marginal vein, which, if existing, runs parallel to the marginal artery
- The pulmonary veins and their pericardial recess may be identified superiorly to the mediastinal sheet
LEFT LATERAL SURFACE
- By lifting the apex from the pericardial cavity and rotating it slightly to the right side, the entire inferior two-thirds of the sternocostal surface and the left margin of the left ventricle may be exposed
- One should be aware that in this exposure, only the proximal course of the OMs is brought into surgical view, and consequently any stenosis or other malformation positioned on the proximal course of the arteries may not be seen.
Exposure of the left lateral surface of the heart, right lateral view
- D2 is seen in its entirety, running parallel to the LAD and terminating at the anterolateral aspect of the sternocostal surface.
- The left marginal artery and its corresponding vein appear lateral and inferiorly, and toward the apex.
- Note that the posterolateral vein appears at the distal left margin of the heart
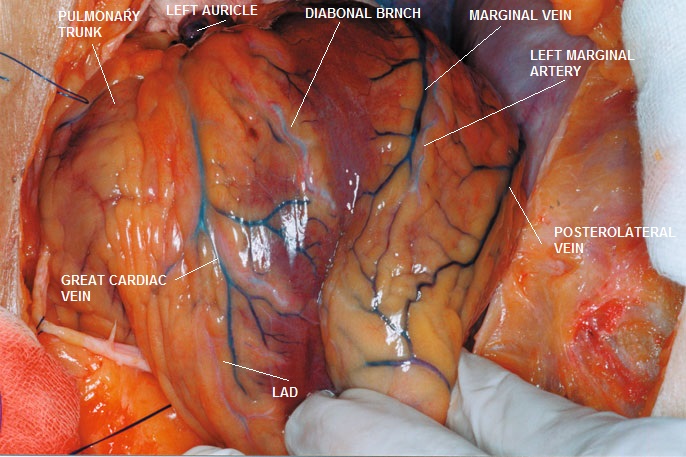
Lateral Surface of the Heart