CONDUIT ANATOMY
INTERNAL THORACIC (MAMMARY) ARTERY
HARVESTING THE IMA
TECHNIQUE
- Median Sternotomy with dissection of the restrosternal and precardial tissue.
- An asymmetric (IMA) sternal retractor used to elevate the hemisternum.
- Table should be turned away from the surgeon and elevated to the appropriate height.
- The pleural reflection may be dissected from the anterior chest wall.
- The pleural space may be opened widely from the apex near the subclavian vein to the diaphragm.
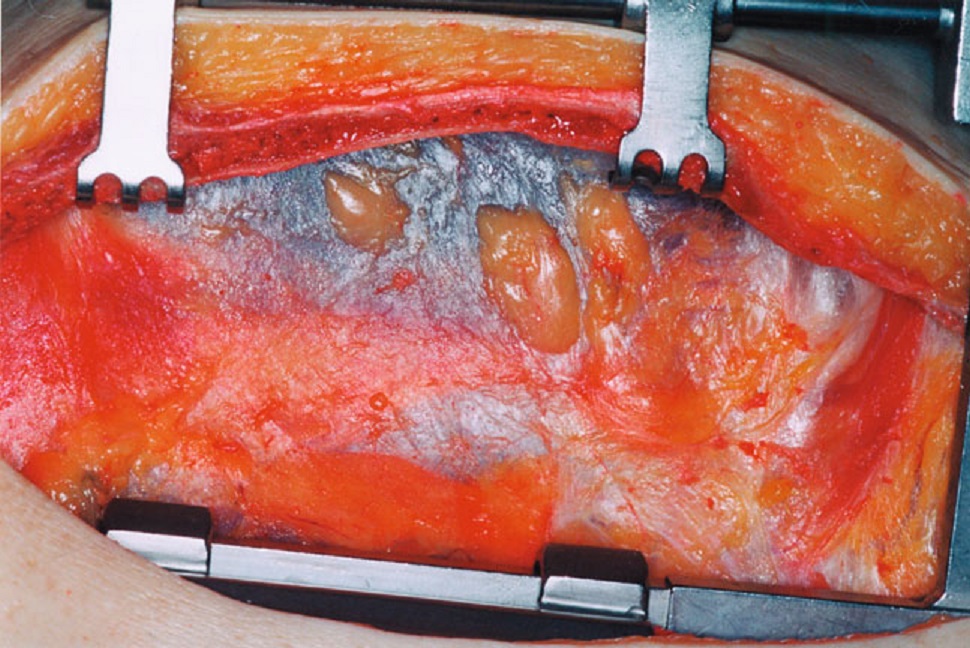
Exposure of the Left Hemithorax
- A large mediastinal branch of the IMA may be detected running toward the precardial fat tissue
- It should be secured with clips to avoid excessive bleeding.
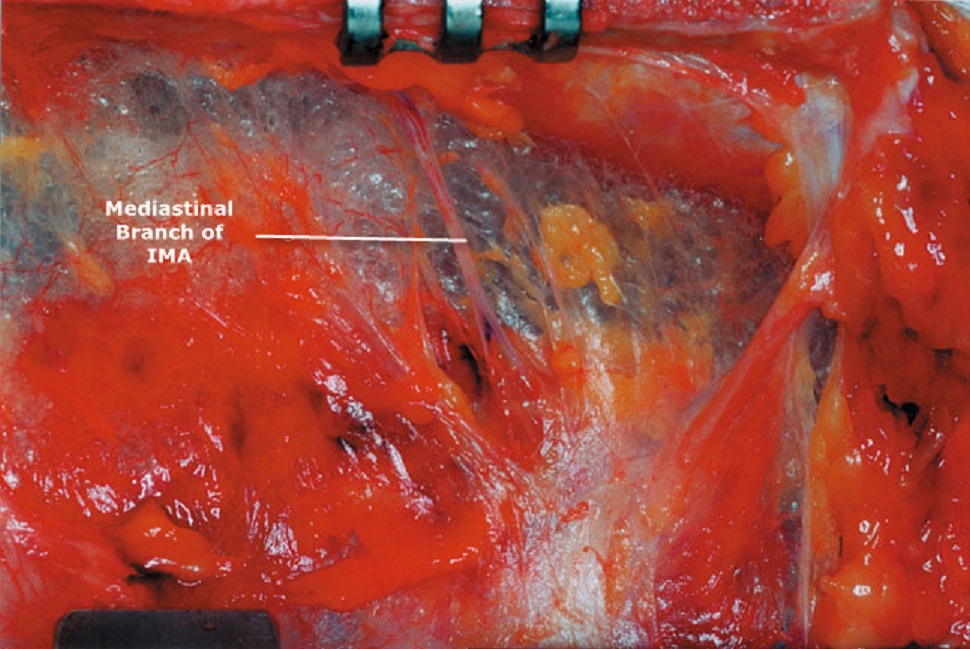
Mediastinal Branch of IMA
- Prior to dissection, IMA should be identified on the internal chest wall.
- IMA runs approximately 1.5 cm lateral to the sternal edge, between two veins.
- Pulsation of the artery may be visualized or manually palpated.
- IMA may be visually identified quite well between the first rib and the third intercostal space where it runs on the parietal pleura.
- From the third rib to its bifurcation, IMA runs between the chest wall and transversus thoracis where artery and the veins cannot be visualized very well and but still can be manually palpated.
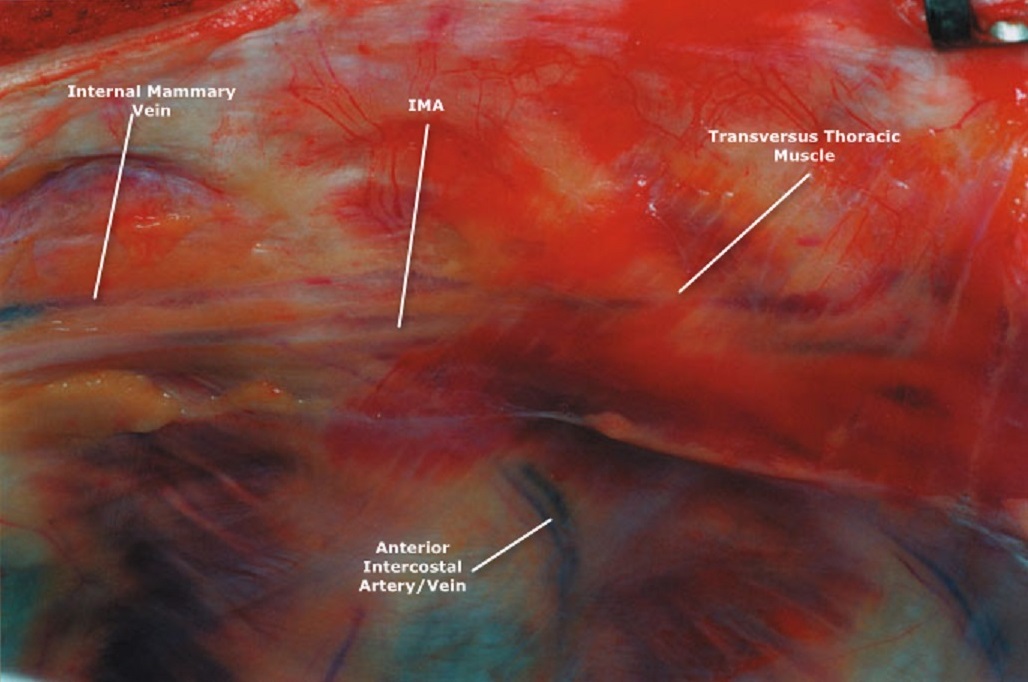
Relation of the internal thoracic artery to the vein
- Some advocate leaving the pleura intact by simply pushing it away from the endothoracic fascia.
- This aims to reduce the incidence of postoperative pleural effusion and hemidiaphragm impairment
- Intraoperatively the intact pleura may retract the lung away from the operating area.
- This tends to displace IMA pedicle and may kink it with the inflation of the upper lobe of the lung.
- The medial aspect of the endothoracic fascia is then incised at most accessible portion of the IMA, usually at the level of the middle or inferior third.
- There are two well-established dissection methods; Skeletonized and Pedicle Harvesting
- The dissection may be started at any point along the IMA
- Care must be taken not to grasp the artery directly; retraction against the vein or fascia is preferable.
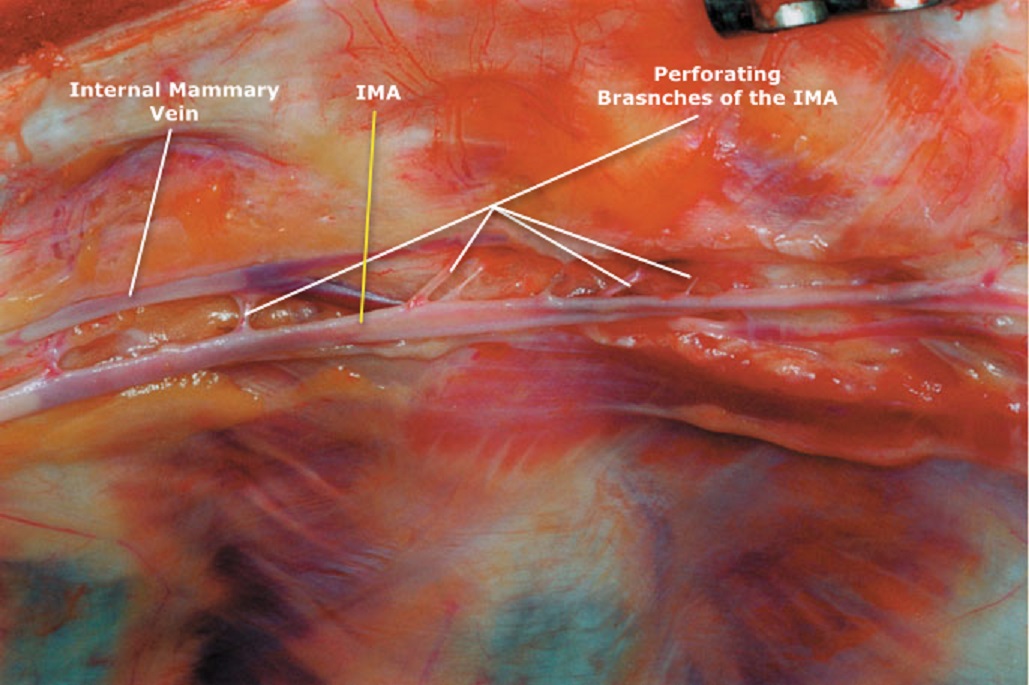
Perforating branches of the internal thoracic artery
Skeletonized Harvesting
- Prior to the incision, the artery has to be identified at the point where it crosses the costal cartilage
- The fascia is incised at the superior-most level of the artery near the internal thoracic vein.
- Downward traction of the fascia with the pedicle, together with cold (blunt) dissection using the electrocautery blade separates the artery from the chest wall, surrounding muscle, fascia.
- Isolate the medial aspect of IMA then progress over the superficial surface toward its lateral side securing its branches with metal clips just over the IMA.
- Dissection is carried out along the entire course of the artery.
Pedicle Harvesting
- A longitudinal fascial incision is made approximately 1 cm lateral and medial to the artery
- The artery is harvested as a pedicle including the fascia, muscle, connective tissue, and both veins
- The incision is made on the cartilage as there are no branches of the artery
- The entire pedicle can be detached from the chest wall
- Sternal perforating and anterior intercostal arteries are cauterized or clipped depending on size
- Downward traction of the pedicle with smooth-tipped forceps and peeling it down from the chest wall by gentle cold dissection with the electrocautery blade and securing the perforating branches
- Permanent downward traction facilitates the distal dissection.
- Finally, the pedicle has been separated from the chest wall.
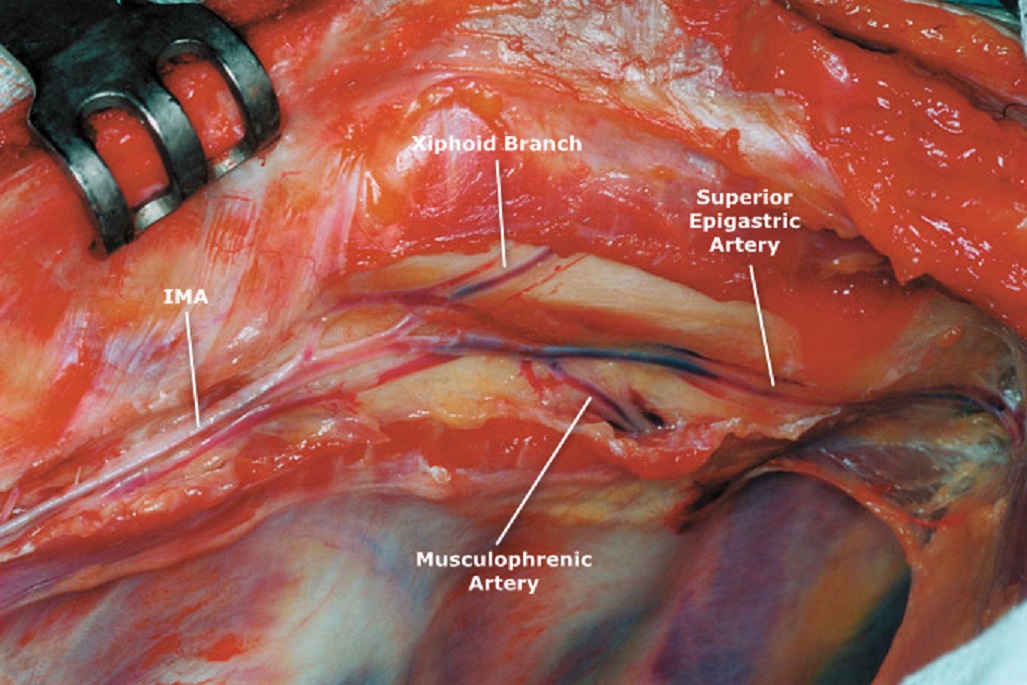
Terminal Branches of the IMA
- Additional length can be obtained by opening the rectus sheath and additional length of vessel may be taken down.
- After an appropriate length is achieved, the distal end of the graft is secured with a clip.
- The dissection is carried on caudally toward the pleural cupule and is followed to its origin at the subclavian artery.
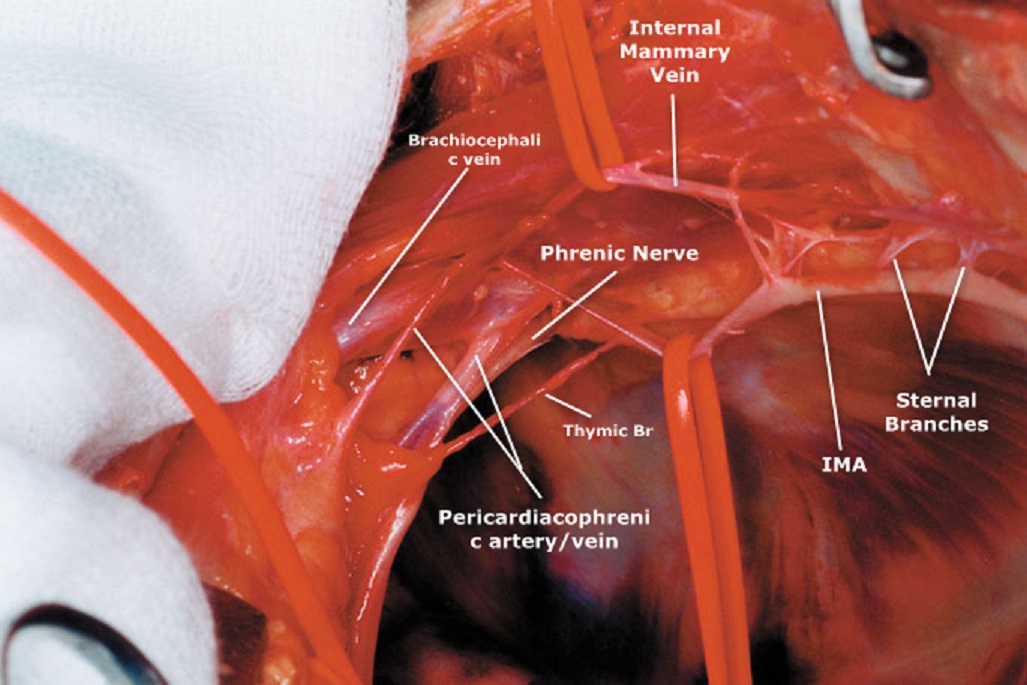
The Proximal Segment of IMA
- Here just in front of the subclavian vein the two branches (the thymic branch and the first intercostal artery must be ligated to avoid the so-called steal phenomenon
- It is important to spare the pericardiacophrenic artery as it is a major blood supply to the phrenic nerve.
- Dissection can be extended upward to its origin between the subclavian vein and the sternohyoid and sternothyroid muscles
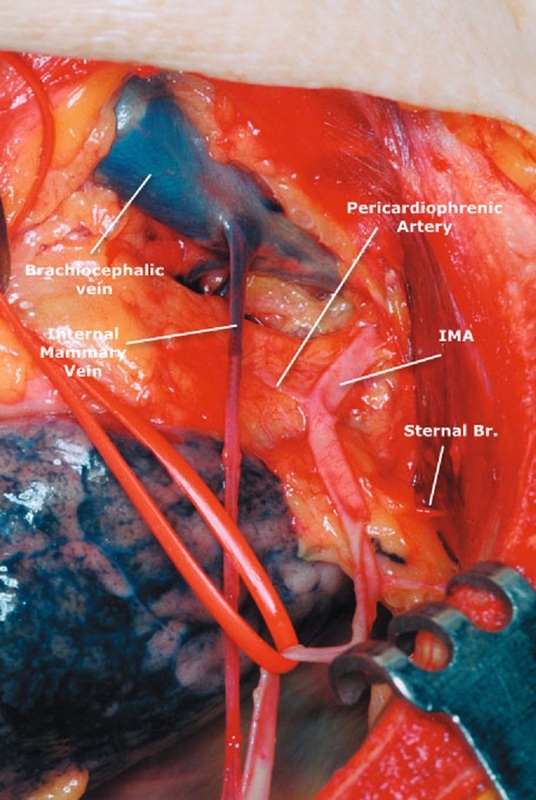
Relationship between the IMA and the brachiocephalic vein
- At this point, the run off of the phrenic nerve cannot be visualized
- On entering the pleural cupule by removing the fatty tissue just behind the brachiocephalic vein, the phrenic nerve comes into view.
- This white cord-like structure runs in front of the artery and crosses it from the lateral to the medial aspect
- Elevation of the subclavian vein using two strings ensures the surgeon great visualization of the origin and topographical relationship of the artery to the phrenic nerve
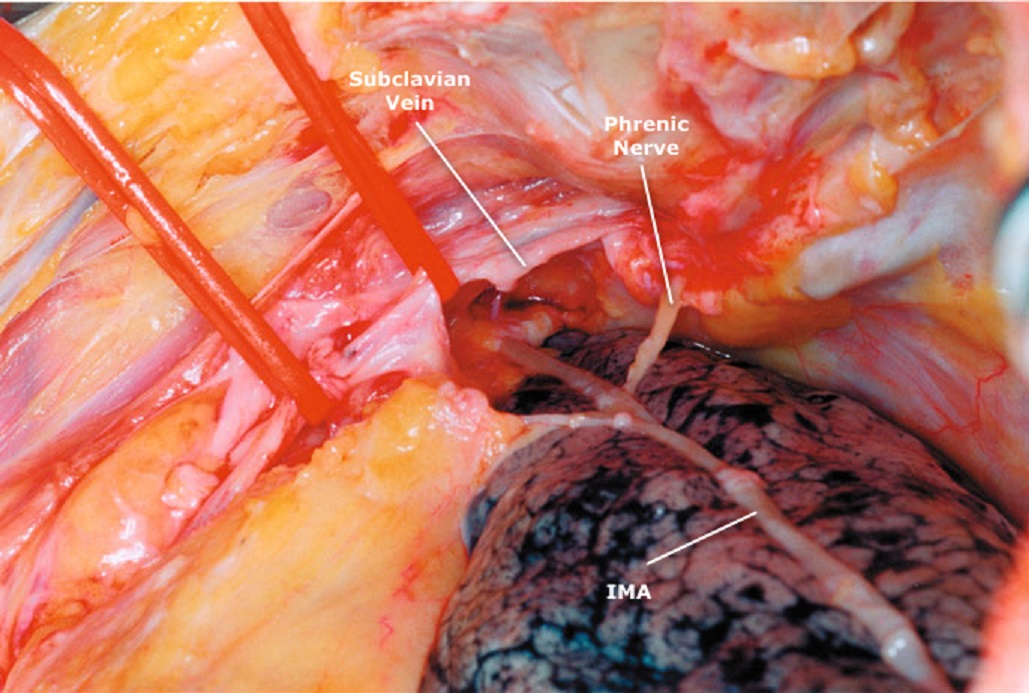
Origin of the internal mammary artery
Bleeding from Mammary Bed