AORTIC VALVE REPLACEMENT
RELATED PROCEDURES
SEPTAL MYOMECTOMY
- Concentric left ventricular hypertrophy in some patients with aortic stenosis.
- It gives echocardiography signs of hypertrophic obstructive cardiomyopathy.
- This asymmetric septal hypertrophy is localized in the subaortic area.
- The occurrence of functional dynamic left ventricular outflow tract obstruction once the aortic stenosis is relieved.
- This is caused by systolic anterior motion (SAM), which is simultaneously also responsible for hemodynamically significant mitral regurgitation.
- Relief of afterload, decrease of preload (hypovolemia), and inotropic medication (catecholamines) are three elementary factors contributing to the onset of this serious complication.
Treatment consists of:
- Alternatively, Alfieri repair, provided the mitral annulus is large enough.
- Rapid volume replenishment.
- Simultaneous catecholamine withdrawal.
- Administration of negative chronotropic and inotropic agents (beta blockers, calcium blockers).
- If no response appears, reoperation is necessary.
- Alternatively, Alfieri repair, provided the mitral annulus is large enough.
Morrow and Brockenbrough Septal Myomectomy
2. Narrow left ventricular outflow tract resulting from asymmetric septal hypertrophy.
- Septal myectomy is to be performed as an adjunct to aortic valve replacement this complication.
- Indicated for AVR in patients with preoperative echocardiography displaying:
2. Narrow left ventricular outflow tract resulting from asymmetric septal hypertrophy.
- After excision of the valve and debridement of the annulus, the septal myectomy is performed.
- Here excision of myocardium from the hypertrophic subvalvular bulk.
- Perforation of the ventricular septum (a rare but serious complication)
- Risk of complete atrioventricular block. (The extent of incision in the rightward direction must not get beyond the midpoint of the right coronary cusp so that the bundle of His is not jeopardized).
- Insufficient extent of the incision in both length and depth may lead to failure of the procedure.
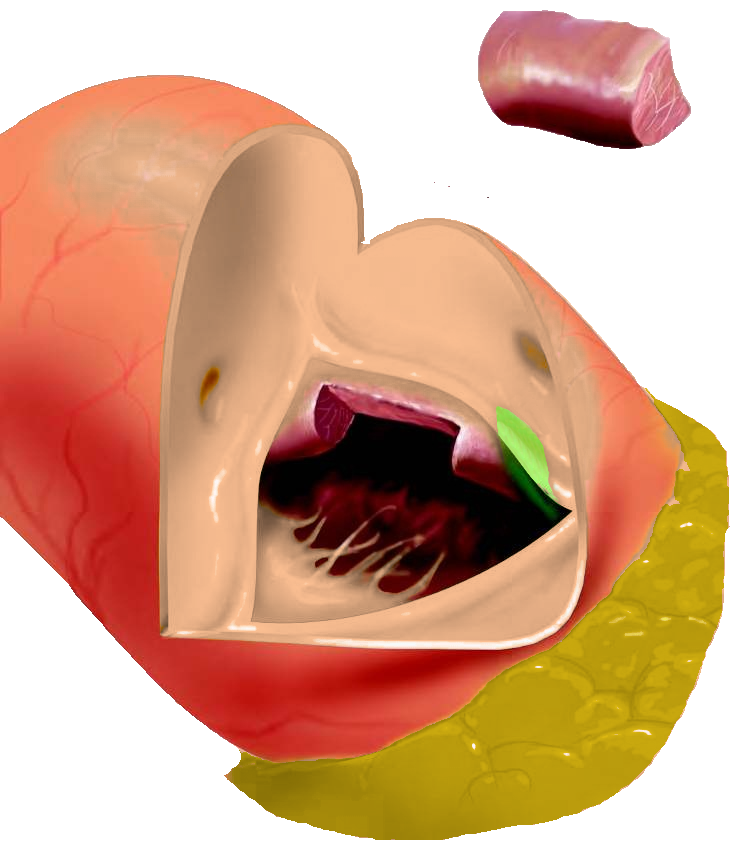
Septal myectomy. Marked in green is the expected course of bundle of His.
(According to Morrow and Brockenbrough)
(According to Morrow and Brockenbrough)
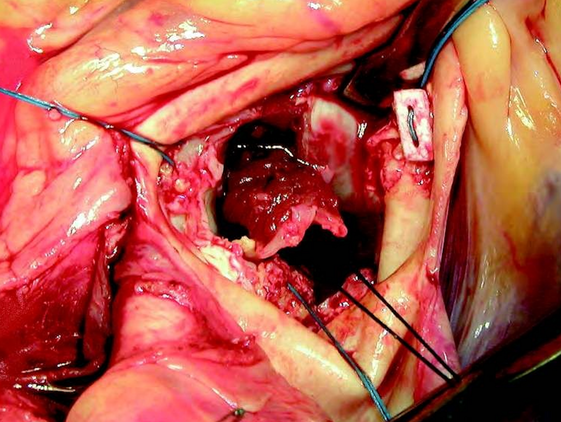
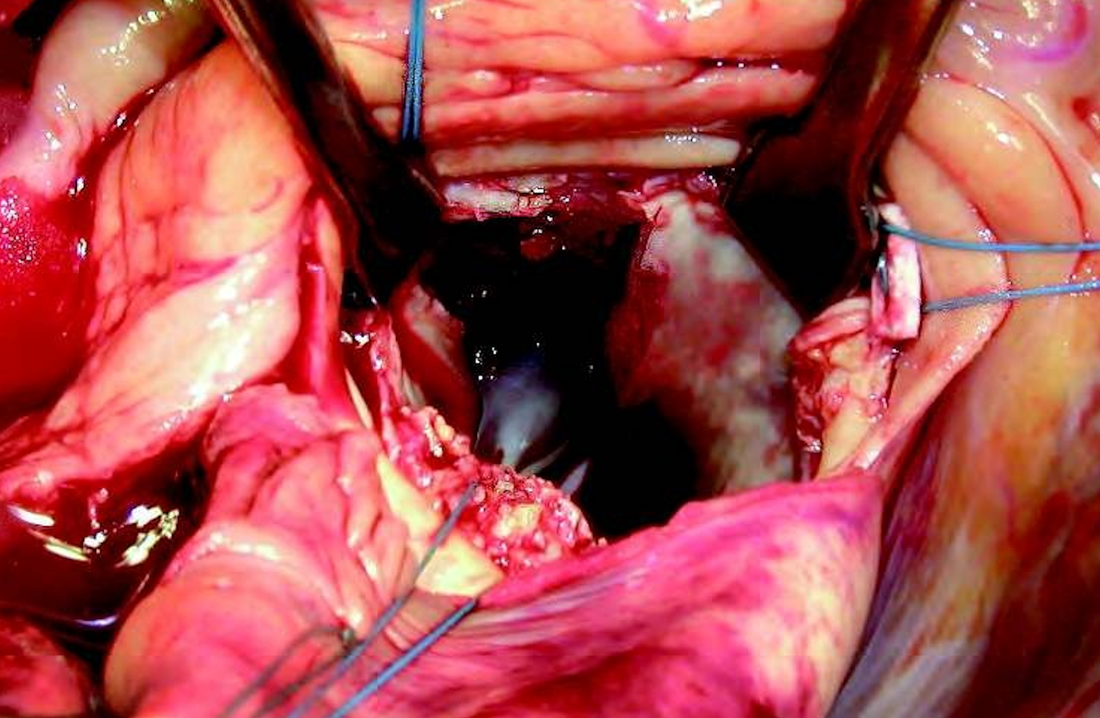
Septal myectomy (operative view).
(According to Morrow and Brockenbrough)
(According to Morrow and Brockenbrough)